Identifying Necrotic Cores (Not lipid Cores) WHICH YOU DON’t use the diffuse borders approach.
We have argue since 1990s diffuse intimal borders do not identify necrotic cores, they are caused by multiple scattering from the intima from structures like calcium deposits or lipid crescents. It is important to understand we aren’t interested in lipid cores as many lipid based structures are stable like PID. We are interested in necrotic cores which have debris which differentiates it from fibrocalcific cores. This is not only important to understanding unstable plaque, it is important for intracoronary imaging and PCI as we (Brezinski group) demonstrated in 2014 when a stent edge ruptured the thin portion of a long necrotic core, it led to core evacuation and a distal occlusion.
JACC 2006 (https://doi.org/10.1016/j.jacc.2005.10.067):
“In a 1990s study, the three plaques were respectively differentiated as: 1) homogeneous, signal-rich region, well-delineated; 2) signal-poor region with sharp borders; and 3) signal-poor region with diffuse borders. Therefore, fibrocalcific and lipid laden plaques are distinguished by the sharp versus diffuse borders; however, this study wa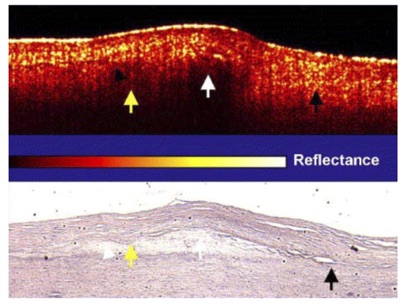 s associated with a high false positive rate, with fibrous caps being diagnosed as lipid laden plaques (sensitivity 71% to 79%). The difficulty in identifying plaque by the diffuse nature of the plaque border is exemplified by figure,from our initial paper published in Circulation on plaque rupture. In this figure, the yellow arrows demonstrate a cap-lipid interface that is diffuse and is covered by a cap with high light scattering (yellow reflections). The white arrow, which is also identifies a region over lipid, identifies a cap-lipid interface that is sharply defined, but the cap is associated with lower scattering. Finally, the black arrow shows an intimal cap that is highly scattering over the intimal-elastic interface (no lipid present). The interface is poorly defined in spite of lack of lipid. The diffuse nature of the intimal-elastin border appears to be that multiple scattering by the cap that is obscuring the border (which would also explain a more rapid local exponential decay). It is unclear, therefore, whether the lipid interface is diffuse in some OCT images because of the core composition, as previously suggested, or multiple scattering from the cap, the latter of which could reduce its predictive power. Future studies are required to establish the mechanism as to why some plaques have diffuse cap/core interfaces”.
s associated with a high false positive rate, with fibrous caps being diagnosed as lipid laden plaques (sensitivity 71% to 79%). The difficulty in identifying plaque by the diffuse nature of the plaque border is exemplified by figure,from our initial paper published in Circulation on plaque rupture. In this figure, the yellow arrows demonstrate a cap-lipid interface that is diffuse and is covered by a cap with high light scattering (yellow reflections). The white arrow, which is also identifies a region over lipid, identifies a cap-lipid interface that is sharply defined, but the cap is associated with lower scattering. Finally, the black arrow shows an intimal cap that is highly scattering over the intimal-elastic interface (no lipid present). The interface is poorly defined in spite of lack of lipid. The diffuse nature of the intimal-elastin border appears to be that multiple scattering by the cap that is obscuring the border (which would also explain a more rapid local exponential decay). It is unclear, therefore, whether the lipid interface is diffuse in some OCT images because of the core composition, as previously suggested, or multiple scattering from the cap, the latter of which could reduce its predictive power. Future studies are required to establish the mechanism as to why some plaques have diffuse cap/core interfaces”.